- Visibility 81 Views
- Downloads 15 Downloads
- DOI 10.18231/j.jdp.2023.008
-
CrossMark

Assessment of mandibular condylar morphology through digital panoramic radiograph: A radiographic study
Introduction
One of the most complex articulations in the human body is the temporomandibular joint (TMJ). It joins the mandible with the skull synchronously and bilaterally. The mandibular condyle, mandibular fossa, and articular eminences of the temporal bone, as well as the soft-tissue elements of the articular disc, its attachments, and the joint cavity, are specific anatomic components of the TMJ.[1], [2]
A mandibular condyle and it's accompanying temporal cavity constitute each joint (glenoid fossa and articular eminence). The TMJ and the tissues that it is connected to are crucial for controlling mandibular mobility and distributing pressures brought on by activities like eating, swallowing, and speaking.[3], [4], [5] A physiological process known as condylar remodelling tries to modify the temporomandibular joint's (TMJ) structure to accommodate the demands of function. It is based on how the condyle's ability to adapt interacts with the mechanical forces supported by the TMJ.
It is believed that the TMJ's components continue to change their structure and morphology even after their ability to grow has stopped.[6], [7] Varied age groups and people exhibit the mandibular condyle in very different ways. Simple developmental variability may cause morphological alterations, as well as condyle remodelling to accommodate developmental variances, malocclusion, trauma, and other developmental disorders and diseases.[8], [9], [10]
Patients with TMJ issues have been advised to use panoramic radiography as a screening technique, and it may be helpful to identify significant bony changes in the condyle.[11], [7] The aim of the current study is to observe and record the variations in condyle forms using an Orthopantomographs (OPGs).
Material and Methods
This retrospective study comprised radiographic evaluation of condylar heads after visualising 200 digitalised OPGs taken for routine investigation. Ethical approval was taken for this study. In the study, patients who underwent conventional OPGs for the diagnosis of surgical (for impacted teeth), or orthodontic issues totaled 200 Orthopantomographs were included. The study excluded patients with a history of trauma to the maxillofacial region, panoramic radiographs showing pathology (osteomyelitis, osteoporosis etc.) in the mandible or maxilla, racture plating, Odontogenic cysts or tumors of the jaws, completely or partially edentulous dental arches, TMJ dysfunction and developmental disorders including hemifacial atrophy and Mandibular condyle imaging affected by a radiography technique error. Radiographs of 117 females and 83 males with ages ranging from 18 to 60 were included in the study.
200 digitalized OPGs were collected for analysis to visualise the radiographic evaluation of 400 condylar heads. Selected digital orthopantomograms (OPG) gave a complete view of the condyle on either side with the best density and contrast. All the OPG’s were taken by Digital Orthopantomograph machine, with exposure conditions of 10 mA and 85 kV Max.
The sample was divided into groups based on age and gender. There were three age ranges determined: (i) Young Adults (18–35 years), (ii) Middle Age (36–55 years), (iii) Older Adults (56 or above).
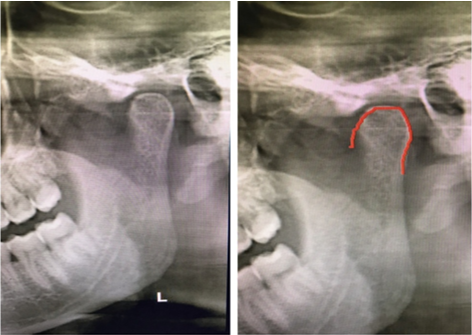
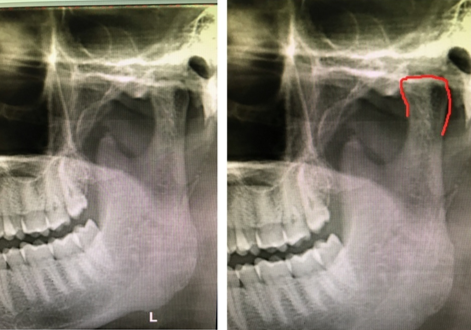
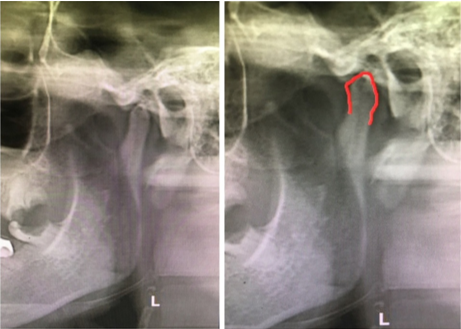
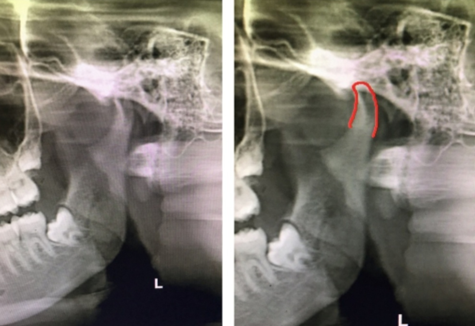
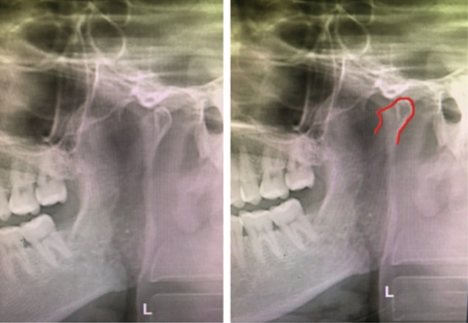
According to Chaudhary et al. (2015) and Gupta A, Acharya G, Singh H, Poudyal S, Redhu A, Shivhare P,[12] the mandibular condyles' morphology was divided into following shapes. ([Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6])
Type I: Oval; Type II: Flattened; Type III: Diamond; Type IV: Crooked finger; Type V:Bifid and Type VI: Bird beak.

The recorded data was then complied and entered in the Microsoft excel; and was analyzed.
Results
Total of 200 OPG’s were studied, out of which 83 were of males and 117 were of females ([Table 1]).
|
Gender |
Frequency |
Percentage |
|
Male |
83 |
41.5 |
|
Female |
117 |
58.5 |
As demonstrated in [Table 2], the majority of participants with radiographs were in Young Adults (18-35 Years) age groups.
|
Gender |
|
Age |
|
|
|
|
Young adults ( 18-35 years) |
Middle age ( 36-55 years) |
Older adults (56 or above) |
Total |
|
Male |
53(63,8%) |
29(34.9%) |
1 (1.2%) |
83 |
|
Female |
88(75.2%) |
27(23.07%) |
2(1.7%) |
117 |
The most common shape of condyle on right observed was oval (43.5%) followed by Bird Beak (20.5%), Diamond (12.5%), Flattened (12%), Crooked finger(6.5%) and Bifid (5%).[[Table 3]]
|
Right condyle |
Frequency |
Percentage |
|
Oval |
87 |
43.5 |
|
Flattened |
24 |
12 |
|
Diamond |
25 |
12.5 |
|
Crooked finger |
13 |
6.5 |
|
Bifid |
10 |
5 |
|
Bird beak |
41 |
20.5 |
|
Total |
200 |
100.0 |
The most common shape of condyle on left observed was Oval (51%) followed by Bird Beak (15%), Diamond (14%), Flattened (9%), Crooked finger(8%) and Bifid (3%).[[Table 4]]
|
Left condyle |
Frequency |
Percentage |
|
Oval |
102 |
51 |
|
Flattened |
18 |
9 |
|
Diamond |
28 |
14 |
|
Crooked finger |
16 |
8 |
|
Bifid |
6 |
3 |
|
Bird beak |
30 |
15 |
|
Total |
200 |
100.0 |
In Males, the commonest form of left and right condylar morphology was Oval and the least form of right condylar morphology was Bifid, whereas the least form of left condylar morphology observed was Bifid and Crooked Finger.[[Table 5]]
|
|
Shape |
|
Right condyle |
Left Condyle |
|
|
Oval |
Number |
36 |
43 |
|
Males |
|
% within males |
43.37 |
51.8 |
|
|
Flattened |
Number |
8 |
6 |
|
|
|
% within males |
9.63 |
7.22 |
|
|
Diamond |
Number |
13 |
12 |
|
|
|
% within males |
15.66 |
14.45 |
|
|
Crooked finger |
Number |
5 |
4 |
|
|
|
% withinmales |
6.02 |
4.81 |
|
|
Bifid |
Number |
3 |
4 |
|
|
|
% within males |
3.61 |
4.81 |
|
|
Bird beak |
Number |
18 |
14 |
|
|
|
% within males |
21.68 |
16.86 |
|
|
Total |
Number |
83 |
83 |
In Females, the commonest form of left and right condylar morphology was Oval and the least form of left condylar morphology observed was Bifid. [[Table 6]]
|
|
Shape |
|
Right condyle |
Left Condyle |
|
|
Oval |
Number |
51 |
59 |
|
Females |
|
% within females |
43.58 |
50.42 |
|
|
Flattened |
Number |
16 |
12 |
|
|
|
%within females |
13.67 |
10.25 |
|
|
Diamond |
Number |
12 |
16 |
|
|
|
% within females |
10.25 |
13.67 |
|
|
Crooked finger |
Number |
8 |
12 |
|
|
|
% within females |
6.83 |
10.25 |
|
|
Bifid |
Number |
7 |
2 |
|
|
|
% within females |
5.98 |
1.7 |
|
|
Bird beak |
Number |
23 |
16 |
|
|
|
%in males |
19.65 |
13.67 |
|
|
Total |
Number |
117 |
117 |
Discussion
The condylar process and mandibular head make up the mandibular condyle. The deepest part of the sigmoid notch is connected to the masseteric tuberosity by an extension line that is referred to as the condylar process and head subunit. The head, neck, and subcondylar region make up the condylar process and head subunit.[13]
When compared to more modern imaging modalities like CT, MRI, and CBCT, maxillofacial radiography using an orthopantamogram is reported to be more affordable and is utilised as a standard screening tool[14], [15] in several sectors of dentistry.[15]
In this study, done in Punjabi population (Northern India), it was observed that the most common shape of the condyle on the right and left side was Oval, which was in accordance with Pranay Ratna et al.’ s study.[16]
In our present study, among males and females, the most common shape of the condyle was Oval on the right and left side. This finding supports the result of previous study[17] by Aqeel Ibrahim Lazim Al-Saedi et al., which also concluded that in both males and females of all ages, the oval shape was the most prevalent.
The least common shapes of condyle noted in our study were bifid and crooked finger, which was similarly seen in the previous study by Singh et al.[18] and Gupta A et al.[12]
The second most common shape of the condyle noted in our study was Bird beak on both the sides, which was at contradiction with the results of the study conducted by Nagaraj et al.,[19] in which flattened shape was noted as the second most common.
The third most common shape of the condyle seen in our study on both the sides was Diamond, which was similar to the study by Sonal et al.[20]
In our study, it was noted that the fourth most common shape of the condyle was flattened.
The three-dimensional TMJ is depicted in two dimensions on radiographs. Therefore, it is necessary to consider several positional aspects as well, especially when considering the anatomical tilt of the condyle. Condyle information can now be obtained in depth using a number of additional modalities, such as cone beam volumetric imaging and CT scan.[21]
Conclusion
This study was done to identify the mandibular condyle's most common radiographic forms on the OPG. In our present study, six different shapes (Oval, Flattened, Bird beak, Diamond, Crooked finger, and bifid) of the condyle is identified, out of which oval shape is the most common on both the sides and is also most common in both the genders. The least common shape of the right and left condyle is Bifid.
Source of Funding
None.
Conflict of Interest
None.
References
- EL Lewis, MF Dolwick, S Abramowicz, SL Reeder. Contemporary imaging of the temporomandibular joint. Dent Clin North Am 2008. [Google Scholar]
- B Singh, NR Kumar, A Balan, M Nishan, PS Haris, M Jinisha. Evaluation of Normal Morphology of Mandibular Condyle: A Radiographic Survey. J Clin Imaging Sci 2020. [Google Scholar] [Crossref]
- GA Zarb, GE Carlsson. Temporomandibular disorders: osteoarthritis. J Orofac Pain 1999. [Google Scholar]
- DM Laskin, W Greenfield, E Gale. Report of the president's conference on the examination, diagnosis, and management of temporomandibular disorders. J Am Dent Assoc 1983. [Google Scholar]
- MK Murphy, RF Macbarb, ME Wong, KA Athanasiou. Temporomandibular disorders: a review of etiology, clinical management, and tissue engineering strategies. Int J Oral Maxillofac Implants 2013. [Google Scholar]
- V Hegde. A review of the disorders of the temperomandibular joint. Journal of Indian Prosthodontist Society 2005. [Google Scholar]
- A L Mathew, A A Sholapurkar, K M Pai. Condylar Changes and Its Association with Age, TMD, and Dentition Status: A Cross-Sectional Study. Int J Dent 2011. [Google Scholar]
- S Standring. . Gray’s anatomy the anatomical basis of clinical practice, (39thedn) 2005. [Google Scholar]
- X Alomar, J Medrano, J Cabratosa, J A Clavero, M Lorente. Anatomy of temporomanidular joint. Seminars in Ultrasound CT and MRI 2007. [Google Scholar]
- Hegde, Shruthi & Bn, Shishir Shetty. . Morphological and Radiological Variations of Mandibular Condyles in Health and Diseases: A Systematic Review 2013. [Google Scholar]
- H C Crow, E Parks, J H Campbell, D S Stucki, J Daggy. The utility of panoramic radiography in temporomandibular joint assessment. Dentomaxillofacial Radiology 2005. [Google Scholar]
- A Gupta, G Acharya, H Singh, S Poudyal, A Redhu, P Shivhare. Assessment of Condylar Shape through Digital Panoramic Radiograph among Nepalese Population: A Proposal for Classification. Biomed Res Int 2009. [Google Scholar]
- K Y Choi, J D Yang, H Y Chung, B C Cho. Current concepts in the mandibular condyle fracture management part I: overview of condylar fracture. Arch Plast Surg 2012. [Google Scholar]
- A L Mathew, A Sholapurkar, K M Pai. Condylar changes and its association with age, TMD, and dentition status: a cross-sectional study. Int J Dent 2011. [Google Scholar]
- Dathar Sahithi, Sudhakara Reddy, D V Divya Teja, Jyothirmai Koneru, Kotu Nagavenkata Sai Praveen, R Sruthi. Reveal the concealed - Morphological variations of the coronoid process, condyle and sigmoid notch in personal identification. Egyptian Journal of Forensic Sciences 2016. [Google Scholar]
- P R Shakya, R Nyachhyon, A Pradhan, R Tamrakar, S Acharya. Morphology of condyle- a radiographic study. Journal of Chitwan Medical College 2022. [Google Scholar]
- Aqeel Al-Saedi, I L Al-Taee, R; Al-Jasim, N H Al-Bakhakh, B. A panoramic study of the morphology of mandibular condyle in a sample of population from Basrah city. Int. J. Morphol 20202. [Google Scholar]
- A Singh, A Gupta, S K Mahanta, D Deepak, K Sonam. . Variations in shapes of mandibular condyles on digital orthopantomograph among patients visiting a dental college 2021. [Google Scholar]
- T Nagaraj, H Nigam, H N Santosh, S Gogula, C K Sumana, P Sahu. Morphological variations of the coronoid process, condyle and sigmoid notch as an adjunct in personal identification. Pathology & Surgery 2017. [Google Scholar]
- V Sonal, P Sandeep, G Kapil, R Christine. Evaluation of condylar morphology using panoramic radiography. Journal of Advanced Clinical & Research Insights 2016. [Google Scholar]
- M M Anisuzzaman, S R Khan, Mti Khan, M K Abdullah, A Afrin. Evaluation of Mandibular Condylar Morphology by Orthopantomogram In Bangladeshi Population. Update Dental College Journal 2019. [Google Scholar]