- Visibility 75 Views
- Downloads 10 Downloads
- DOI 10.18231/j.jdp.2023.030
-
CrossMark

Congenitally missing bilateral maxillary lateral incisors – (A Developmental Anomaly) restored with implants and crowns followed by orthodontic treatment
Introduction
Bilateral – Missing maxillary posterior teeth are a rare developmental anomaly that impacts the esthetics, phonetics and confidence of young people and becomes a difficulty for dentists to correct. Understanding the complexity of tooth development, it is the unique part of the human body A complex interaction between the tooth epithelium and the underlying ectomesenchyme leads to successful tooth development.[1] The interaction between molecular signals, receptors and transcription control systems is a complex process, failure of which can lead to tooth loss. It is known that more than 300 genes responsible for odontogenesis are expressed in teeth. Genetics play an important role in congenital genesis, as studies on identical twins confirm. Here we report a case with bilateral congenital missing upper lateral incisors. [2] The best way of replacing the congenital missing teeth were using dental implants and crowns in means of esthetics, phonetics and mastication. [3]
Case Report
A 23-year-old woman presented to our clinic with a four-year history of a major complaint of tooth gaps in the upper anterior region. She gave no details on the extractions. Medical history and dental history were not linked. No abnormalities were found extraorally. On intraoral examination, it was found that the upper right and left lateral incisors were missing. On clinical examination, a congenital absence of the upper left and right lateral incisors was revealed. An intraoral periapical radiograph of the maxillary bilateral lateral incisors was taken, which confirmed the diagnosis of congenital absence of maxillary bilateral lateral incisors. The treatment plan was established as needed, the patient was referred to the ortho-pantomograph (OPG) and orthodontic evaluation and esthetic correction were recommended. Orthodontic treatment was performed to correct the angles of the migrated canines and central incisors and to replace the missing bilateral lateral incisors.
After the orthodontic corrections of occlusion, we replaced her lateral incisors with the help of endosseous implants followed by the crowns for the same.
Surgical Porcedure
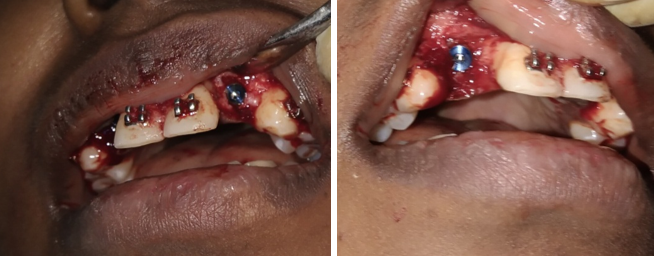
The patient was explained the current clinical situation, the treatment plan and the procedure. The patient was recommended to have routine laboratory tests such as bleeding time, clotting time, hemoglobin count and complete blood count. After obtaining the informed consent and all diagnostic aids from the patient, treatment was initiated. 2% lignocaine 1:80,000 was administered on infiltration technique in relation to 12 and 22 regions. After signs of complete anesthesia, the incisions were placed and flap reflection done to expose the bone. Then the implant site preprations were done using the drills, after the osteotomy site preparation implants were placed at respective sites.
No bleeding was observed, after which stitches were applied. The patient was prescribed analgesics and antibiotics, one capsule of amoxicillin (500 mg) three times a day for 3 days and one nonsteroidal anti-inflammatory tablet of ibuprofen (400 mg) + paracetamol (325 mg) three times a day for 3 days checked for suture removal after a week.
Healing was uneventful. The patient reported after 4 months for a prosthetic crowns. After taking the radiograph we proceed with the crowns. This improves the esthetics, phonetics and mastication which make the patient smile confident.
Clinical Pictures




Discussion
Congenitally missing teeth are a result of disorders in the early stages of development and are suspected to be a mild dysplastic expression of the ectoderm. [4] The prevalence may be increasing, possibly due to evolutionary changes or due to increasing diagnoses. [5] The etiology of congenitally missing teeth includes trauma, infection, drugs, and genetic factors. As previously mentioned, genes play an important role in tooth aplasia. [6] The most supported etiological theory postulates a polygenic mode of inheritance, in which epistatic genes and environmental factors exert some influence on the phenotypic expression of the genes involved, resulting in tooth germ in the initial stages of formation, i. H. of initiation and proliferation. [7] Most authors observed a predominance of bilateral missing teeth to an extent that was about twice that of unilateral missing or even three times that of unilateral missing. Gender could be a risk factor for tooth agenesis. Females tend to be more affected and the male to female ratio is around 2:3. Some authors examined the teeth individually and found significant sexual dimorphism only for certain teeth, such as the upper incisors and upper first premolars, all on the right side only. [8] Of these teeth, only the upper right central incisor was missing more often in males, while the other teeth were more common in females. [9]
The most common congenital missing permanent teeth, excluding the upper and lower third molars, are the mandibular second premolars, followed by the maxillary lateral incisors and the maxillary second premolars. [10] Correcting aesthetics is of paramount importance, whether through orthodontic or prosthetic treatment. [11] In the above case, orthodontic correction followed by prosthetic restoration was recommended.
There are differences in regard to root angulation and parallelism between congenitally missing teeth and missing teeth that existed at one time and were subsequently lost. [12] In the situation of a congenitally missing tooth, the neighboring teeth erupt into the space of the missing tooth and therefore can be parallel or even convergent to the other teeth.[13] This situation requires important root control during the space opening phase of orthodontics and must be monitored radiographically. [3]
Conversely, the changes that accompany the loss of a tooth include tipping or drifting movements of the remaining teeth. The correction for this situation orthodontically usually entails a much simpler tipping or uprighting movement, which is much more easily accomplished than a translation or root torquing movement. [6]
Conclusion
Treating any developmental anomaly is a challenging task, but thanks to the great advances in dental implants and crowns and proper oral hygiene and care these days, it has hardly got any easier.[14] The addition of chlorhexidine mouthwash to maintenance therapy provides dental implants with a good plaque control.[15]
Source of Funding
None.
Conflicts of Interest
There are no conflicts of interest.
References
- NI Pini, LM Marchi, RC Pascotto. Congenitally missing maxillary lateral incisors: update on the functional and esthetic parameters of patients treated with implants or space closure and teeth recontouring. Open Dent J 2015. [Google Scholar] [Crossref]
- I Thesleff. Epithelial–mesenchymal signalling regulating tooth morphogenesis. J Cell Sci. 2003; 116: 1647-1648 . J Cell Sci 2003. [Google Scholar] [Crossref]
- R Fürhauser, D Florescu, T Benesch, R Haas, G Mailath, G Watzek. Evaluation of soft tissue around single-tooth implant crowns: The pink esthetic score. Clin Oral Implants Res 2005. [Google Scholar] [Crossref]
- I Thesleff, S Keranen, J Jernvall. Enamel knots as signaling centers linking tooth morphogenesis and odontoblast differentiation. Adv Dent Res 2001. [Google Scholar] [Crossref]
- D Militi, A Militi, M C Cutrupi, M Portelli, L Rigoli, G Matarese. Genetic basis of non syndromic hypodontia: a DNA investigation performed on three couples of monozygotic twins about PAX9 mutation. Eur J Paediatr Dent 2011. [Google Scholar]
- A Fekonja. Hypodontia in orthodontically treated children. Eur J Orthod 2005. [Google Scholar] [Crossref]
- N Mattheeuws, L Dermaut, G Martens. Has hypodontia increased in Caucasians during the 20th century? A meta-analysis. Eur J Orthod 2004. [Google Scholar] [Crossref]
- I Thesleff. The genetic basis of tooth development and dental defects. Am J Med Genet A 2006. [Google Scholar] [Crossref]
- I Thesleff. Genetic basis of tooth development and dental defects. Acta Odontol Scand 2000. [Google Scholar] [Crossref]
- R Silva Meza. Radiographic assessment of congenitally missing teeth in orthodontic patients. Int J Paediatr Dent 2003. [Google Scholar] [Crossref]
- I Peker, E Kaya, S Darendeliler-Yaman. Clinic and radiographical evaluation of non-syndromic hypodontia and hyperdontia in permanent dentition. Med Oral Patol Oral Cir Bucal 2009. [Google Scholar]
- V Rakhshan. Congenitally missing teeth (hypodontia): A review of the literature concerning the etiology, prevalence, risk factors, patterns and treatment. Dent Res J 2015. [Google Scholar] [Crossref]
- M Bahrami, FS Saber, A Hendi. Comprehensive Treatments for Congenitally Missing Teeth and Generalized Diastema. Case Rep Dent 2017. [Google Scholar] [Crossref]
- R Fürhauser, D Florescu, T Benesch, R Haas, G Mailath, G Watzek. Evaluation of soft tissue around single-tooth implant crowns: the pink esthetic score. Clin Oral Implants Res 1012. [Google Scholar]
- M Addv. The use of antiseptics in periodontal therapy. Clinical Periodontology and Implant Dentistry. 4th Edn. 2003. [Google Scholar]