- Visibility 715 Views
- Downloads 32 Downloads
- Permissions
- DOI 10.18231/j.jdp.2024.040
-
CrossMark

Inclination of retromolar pad and its relationship to occlusal plane in edentulous subjects: An observational study
Abstract
Introduction: The muscle attachments and strong cortical bone beneath, the retromolar pad (RMP) make it least in resorption than the bony mandibular residual alveolar ridge. The stock trays are typically flat for resorbed ridges that put excessive strain on the RMP region, stock trays frequently need to be modified arbitrarily. Also various studies are conducted on relationship of retromolar pad to occlusal plane on dentulous subjects but less on edentulous subjects. So, this study is conducted to record the angular dimensions of retromolar pad to residual ridge and its relation to occlusal plane.
Aim & Objectives: To determine the angle made by slope of retromolar pad with crest of ridge and its relationship to occlusal plane.
Materials and Methods: On 80 study (40 male and 40 female subjects) master casts, RMP inclines and residual ridge crests were marked with markers. The angle between the slope of retromolar pad and crest of ridge were then measured using a protractor that was kept at eye level. To check relationship of retromolar pad to occlusal plane a metallic scale is used by dividing the retromolar pad into three zones (upper, middle and lower third).
Results: The angle made by slope of retromolar pad with crest of ridge is measured in range of 123-167 on right side and 112 -173 degrees left side in female subjects and 105-175 degrees on right side and 125-173 on left side male subjects. An occlusal plane was checked intraorally and extraorally on cast by sliding scale on occlusal rim. The scale coincides at the point of junction of upper third and middle third extending the level of plane of occlusal rim in more than half of selected subjects. The paired sample t-test gave a p-value of 0.048. The mean angle obtained was 146+ _ 12.36 in male and 150+ - 14.87 degrees in female subjects to which stock metal tray can be incorporated.
Conclusion: The present study demonstrated a mean angle of 146 degrees in male and 150degree in female subjects which would be adequate to accommodate higher angles upto 175 degrees in both the subjects. This mean angle can be considered as standard angle for incorporation in stock metal tray for fabrication of complete dentures. Also the present study demonstrated the junction of upper third and middle third of retromolar pad is considered as safer option in determining occlusal plane in mandibular arch and its relationship to occlusal plane due to its least resorption than mandibular residual alveolar ridge.
Introduction
Retromolar pad (RMP) are pear-shaped, soft, and glandular pads that are inserted into the oral mucosa at the distal third molar region of mandibular residual ridge.[1], [2], [3], [4] Retromolar pad is glandular tissue with buccinator muscle fibres, superior constrictor muscle fibres and Pterygomandibular raphe , tendon of temporalis muscle. [1], [2], [3], [4], [5] The mandibular resorption rate is four times more than the maxilla, due to extreme residual ridge resorption, there is significantly reduced surface area, transformed facial esthetics, the altered vertical dimension of occlusion, and an interarch relationship thus compromising stability,retention. [6], [7], [8], [4]
Due to the attachments of these muscles and dense cortical bone underlying the retromolar pad makes retromolar pad relatively resistant to resorption. [1], [7], [4], [5] So in cases with extremely resorbed ridges Retromolar pad can be considered relatively stable posterior landmark . [1], [9], [7], [4] The residual ridge anterior to the retromolar pad is firm whereas the pad consists of displaceable tissue which compromises stability when masticatory load is directed towards the pad. [1], [9], [7], [10] So tooth should not be placed in that region during fabrication of complete denture. [9], [7], [10] The denture base should extend up to approximately half to two thirds of the retromolar pad as incomplete coverage will cause step like defect anterior to pad. [1], [7] So height of the denture base that covers the pad should be shortened avoiding the interference during the translatory movements (protrusion and lateral excursions) and also tissue trap between denture base and mucosa. [9], [7]
When the denture border crosses its surface retromolar pad acts as cushion and provides excellent seal and stability by resisting movements against displacement. [1], [2], [3] Retromolar pad is one of the most reliable guides for the arrangement of the mandibular teeth in the complete denture and dictates the posterior occlusal plane as mandibular first molar corresponds to the level of halfway up to two thirds of the height of the retromolar pad. [1], [9], [2], [11], [4]
The slope of retromolar pad to the crest of ridge should be recorded properly as it is an angle that the retromolar pad makes with the residual alveolar ridge. [1], [7] This angle prevents posterior displacement of the denture in extremely resorbed ridges. [1] A line is drawn on the cast from the lingual surface of the retromolar pad, passing anteriorly lingual to the crest in the premolar region and establishes the lingual extent of the occlusal rim. [1] This line determines the position of lingual surfaces of the mandibular posterior teeth. [1]The lower denture teeth must end just before the residual ridge slopes vertically towards the retromolar pad.[1], [9] So the existing stock trays often require modification to avoid pressure in this region which lead to soreness and rebound effect leading to instability of lower denture. [1], [7]
The level of the occlusal plane is one of the key factors governing occlusal balance and phonation.[12], [13] The occlusal plane of the lower denture should be placed similar to that of the natural teeth so that the tongue and cheek conditioned to function normally at this level.[12], [13] There are different methods for the orientation of the occlusal plane.[14], [13], [15] The occlusal plane lost in edentulous cases should be relocated in complete dentures in terms of function, esthetic and speech to render them satisfactorily. [12], [13], [15] In the anterior region, the occlusal plane is established according to aesthetic and phonetic criteria. [16], [15] There are several landmarks to define the level of occlusal plane posteriorly. [12], [14] The plane, which was previously occupied by the natural teeth, should be as near as with position of occlusal plane in complete denture patients. [17], [13], [11] There are various studies by various authors of different landmarks of retromolar pad and accuracy for orientation of occlusal plane in an edentulous subject. [17], [13], [11], [3]
So, the aim of this study was to record the angle formed by the slope of retromolar pad to crest of residual alveolar ridge in resorbed cases, and to incorporate it in stock trays so that this angle can be considered as standard angle while recording the impression without causing undue pressure on RMP region. This study also aimed to record relation of retromolar pad to occlusal plane.
Materials and Methods
Impression compound, Impression plaster, green stick compound, DPI impression paste, Dental stone type III
Equipments
Metallic Scale: A thin 6” stainless steel scale was used to relate the occlusal plane to the retromolar pad.
Protractor: is used to check inclination of RMP to residual ridge.
Method
The present study demonstrates the angle formed by the retromolar pad with the residual alveolar ridge. 80 mandibular master casts of edentulous patients with 40 male and 40 female selected.
Inclusion criteria
Completely edentulous patients of both the genders with well healed ridges and also patients consenting to participate in the study.
Exclusion criteria
Patients with unhealed extraction sockets or history of recent extraction, patients with neuromuscular disorder, patients with partially edentulous mandible and patients with a history of maxillofacial trauma and mandibular fracture.
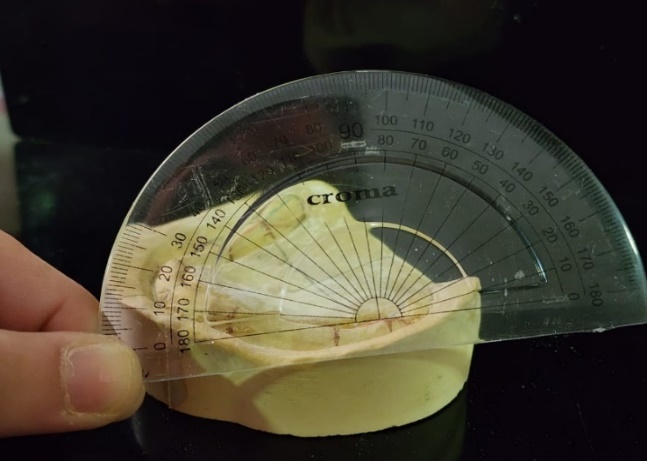
On each master cast, a line was marked using different colored markers, one over slope of retromolar pad and the other over the crest of the distal ridge joining with the retromolar pad ([Figure 1]). The retromolar pad is divided into three regions upper third, middle third and lower third (Figure). Then using protractor at the level of eye the angle formed by joining the slope of retromolar pad with crest of ridge was measured ([Figure 1], [Figure 2]). It was observed that more the residual ridge resorption, more the angle will be steeper.



For determining occlusal plane after taking vertical relation the base plate and occlusal rim is fabricated over each master cast. The stainlesssteel scale is then slided on the occlusal rim posteriorly to make contact with the retromolar pad on the cast extraorally and also checked intraorally in study subjects ([Figure 3]). Occlusal plane was also checked during denture delivery using stainless steel scale ([Figure 4]). The zone of contact at the junction of upper third and middle third of the retromolar pad coincides with the level of occlusal plane of mandibular arch in more than half of the selected subjects including both genders.
Result
The Statistical product and service solution (SPSS) version 22 software was used for all the data calculations and statistics. The mean RMP angle of male subject was 146 ± 12.36 degrees and it was 150.27 ± 14.87 degrees for female subjects. The paired sample t-test gave a p-value of 0.048, which suggested a statistically significant difference. Irrespective of minor differences in RMP angle between male and female subject, mean angle of both genders can be incorporated in stock trays considering it as standard angle. ([Table 1])
|
Angle |
Side |
Range (Degrees) |
Mean ± standard deviation (Degrees) |
Mean ± Standard Deviation of right and left side (Degrees) |
P value (Male vs Female) |
|
Male |
Right |
105-175 |
143±11.6 |
146 ± 12.36 |
p =0.048* (significant difference) |
|
Left |
125-173 |
147±13.8 |
|||
|
Female |
Right |
123-167 |
148±14.7 |
150 ± 14.87 |
|
|
Left |
112 -173 |
151±15.9 |
Discussion
Various factors influence the chronic remodeling process of the edentulous Jaw like gender, genetics, systemic conditions, sequence of tooth loss, length of edentulism ,duration of denture wear, and other unknown factors. [1], [18], [11] This resorptive pattern is limited and the entire edentulous mandibular body has never been known to completely resorb. [18], [11] The mylohyoid muscles , the buccinator muscles , and the additional muscles that surround the mandible are some of the factors that limit chronic bone resorption of the edentulous jaw. [18], [11]
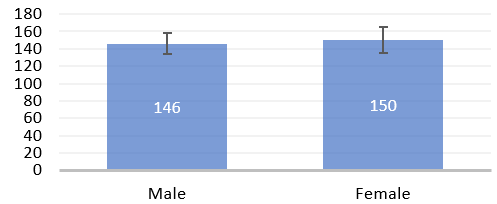
After the loss of distal most tooth, there is remodelling of surrounding bone to merge with the retromolar pad.[1] The retro molar pad should be incorporated within the perimeter of the final impression as it provides excellent basal seal and stability when denture border crosses its surface. [1], [9], [8] The inclination of retromolar pad provides resistance to posterior displacement of denture. [1], [8], [16] Present study reported the most acute angle of 146 degrees( lower limit considering for both genders) between slope of RMP and crest of residual alveolar ridge, which can be considered as the standard angle for the stock trays. [1] ([Figure 5]) shows mean angle for male subjects 146 degree and more in female subjects that was 150 degree, showing significant values .Thus avoiding the necessity to modify stock tray during impression and avoiding undue pressure and soreness on retromolar pad. [1], [9] Due to lack of reproducible reference structures for determining the orientation and position of occlusal plane, different authors use different landmarks and methods to establish the occlusal plane. [16] To validate the relationship between various intraoral landmarks with the occlusal plane of lower denture various studies were conducted suggesting that lower denture occlusal plane should be similar to that of natural tooth occlusal plane for functional efficiency. [9] So there are various studies and literature to support but varies in determining the exact occlusal plane.[16] In the present observational study junction of upper third and middle third of retromolar pad coincides with occlusal plane of mandibular arch in more than half of selected subjects as denture was stable with patient satisfaction (no soreness and pressure) and with good retention after denture delivery.
Conclusion
The stock trays modification provides a mean to record this standard angle which will help in fabrication of good complete denture prosthesis in patients with extremely resorbed completely edentulous mandibular ridges.
The position of the retromolar pad remains almost unchanged, though different proportions of the pad are related to the occlusal plane. The zone of contact of upper third and middle third is relatively safer option in determining the occlusal plane. Though majority of the subjects (75%) showed the occlusal plane at the level of this point of landmark (junction of upper third and middle third) of retromolar pad area with excellent retention and stability, the occlusal plane should be determined by the dynamics of function and not by any particular static relationship. It is also advisable that occlusal plane should also be determined on the basis of anatomical landmarks, esthetics, phonation, comfort and function. So further studies are recommended in determining relation of retromolar pad to occlusal plane, governing all the factors.
Source of Funding
None.
Conflict of Interest
None.
References
- Verma N, Singla S, Sehgal K, Kumar L, Kumar R. Angular Dimensions of Retromolar Pad: An Observational Study. RGUHS J Dent Sci. 2023;15(2):113-5. [Google Scholar]
- Haines R, Barrett S. The structure of the mouth in the mandibular molar region. J Prosth Dent. 1959;9(6):962-74. [Google Scholar]
- Winkler S. . Essentials of complete denture prosthodontics. 1979;253:253-4. [Google Scholar]
- Bernarda L, SI, CM, SC. Biomethrics study of retromolar pad. Int J Odontostomat. 2008;2(1):39-42. [Google Scholar]
- Edwards L, Boucher C. Anatomy of the Mouth in Relation to Complete Dentures. J Am Dent Assoc. 1942;29(3):331-5. [Google Scholar]
- Sharma A, Deep A, Siwach A, Singh M, Bhargava A, Siwach R. Assessment and evaluation of anatomic variations of retromolar pad: a cross sectional study. J Clin Diagn Res. 2016;10(5):143-5. [Google Scholar]
- Verma N, Sehgal K, Sahore P, Khanna M. Categorization of Extremely Resorbed Mandibular Edentulous Ridges and Formulation of Edentulous Stock Trays Conforming to Different Resorbed Ridge Forms: An Observational Study. In J Prosthod Restor Dent. 2023;13(2):70-5. [Google Scholar]
- Wright C. Evaluation of the factors necessary to develop stability in mandibular dentures. J Prosthet Dent. 1966;16(3):414-30. [Google Scholar]
- Dathan P, Nair KC, Jayakumar A, Ajithan L. The validity of retromolar pad as an intraoral landmark in the fabrication of complete dentures-a short review. Acta Scientific Dent Sci. 2021;5(8):48-51. [Google Scholar]
- Jayaram B, Shenoy K. Analysis of mandibular ridge resorption in completely edentulous patients using digital panoramic radiography. J Dent Med Sci. 2017;16(8):66-73. [Google Scholar]
- Ismail Y, Bowman J. Position of the occlusal plane in natural and artificial teeth. J Prosthet Dent. 1968;20(5):407-11. [Google Scholar]
- Gupta R, Aeran H, Singh SP. Relationship of anatomic landmarks with occlusal plane. J Indian Prosthodontic Soc. 2009;9(3):142-7. [Google Scholar]
- Javid N. A technique for determination of the occlusal plane. J Prosthet Dent. 1974;31(3):270-2. [Google Scholar]
- Augsburger R. Occlusal plane relation to facial type. J Prosthetic Dent. 1953;3(6):755-70. [Google Scholar]
- Celebric A, Valentic M, Kralijevic K, Brkić H. A study of the occlusal plane orientation by intra-oral method (retromolar pad). J Oral Rehabil. 1995;22(3):233-6. [Google Scholar]
- Jamie P, Israel K, Baruch A. Retromolar ridge in edentulous patients: clinical considerations. J Prosthodont. 2007;16(6):502-6. [Google Scholar]
- Shetty S, Zargar NM, Shenoy K, Rekha V. Occlusal plane location in edentulous patients: A review. J Indian Prosthodont Soc. 2013;13(3):142-8. [Google Scholar]
- Gruber H, Solar P, Ulm C, Watzek G. Maxillomandibular anatomy and patterns of resorption following atrophy. Endosseous Implants. Scientific and Clinical Aspects. 1993. [Google Scholar]